Drooling during sleep is often treated as a minor, slightly embarrassing occurrence, but from a biological perspective it is a surprisingly informative window into how the human body behaves during rest. What seems like a simple overflow of saliva is actually the result of multiple systems working differently once consciousness fades. The brain, muscles, nervous system, and respiratory pathways all shift into a different mode of operation at night, and drooling can emerge as one of the visible side effects of that transition.
To understand why drooling happens, it is important to first recognize that saliva production never actually stops. The salivary glands continuously produce fluid throughout the day and night, controlled by the autonomic nervous system. While awake, swallowing happens automatically and frequently, guided by both voluntary and reflexive control. The brain constantly coordinates tongue movement, throat muscles, and jaw position to ensure saliva is directed safely into the digestive system. This coordination is so seamless during wakefulness that most people are unaware of it.
When sleep begins, however, the body undergoes a systematic reduction in conscious motor control. This transition is not abrupt but occurs in stages, each associated with different levels of brain activity and muscle tone. As sleep deepens, the brain reduces its monitoring of external bodily functions and prioritizes internal repair processes. One of the first noticeable changes is the relaxation of skeletal muscles, including those in the jaw, cheeks, and tongue. As these muscles relax, the mouth may open slightly, creating a pathway for saliva to escape instead of being swallowed.
This process becomes particularly noticeable during deeper stages of non-rapid eye movement (non-REM) sleep. Non-REM sleep is divided into several phases, with the deepest stage often referred to as slow-wave sleep. During this phase, the body is in its most physically restorative state. Heart rate slows, breathing becomes more regular, and muscle tone is significantly reduced. It is in this state that drooling is most likely to occur, because the coordination required to maintain a sealed mouth and regular swallowing is partially reduced.
REM sleep adds another layer of complexity. During rapid eye movement sleep, brain activity increases and resembles waking patterns in some respects, especially in terms of dreaming and emotional processing. However, the body simultaneously enters a state of muscle atonia, a temporary paralysis of most voluntary muscles. This mechanism prevents people from physically acting out their dreams. While major muscle groups are inhibited, subtle relaxation of facial and oral muscles can still occur, allowing saliva to accumulate and occasionally escape from the mouth.
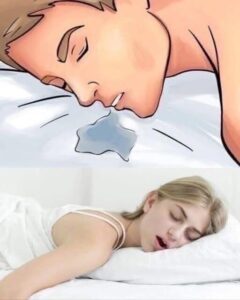
Sleep position plays a major role in whether drooling becomes visible. Gravity has a direct influence on fluid movement in the body, and when a person sleeps on their side or stomach, saliva is more likely to flow outward due to the angle of the mouth. Side sleeping is particularly associated with drooling because one side of the face is partially directed downward. In contrast, back sleeping can reduce drooling because saliva is more likely to remain pooled at the back of the mouth and be swallowed unconsciously, although this position may introduce other factors such as snoring in some individuals.
Breathing patterns are another critical factor. Nasal breathing is the body’s preferred method of respiration during sleep, but when nasal passages are blocked due to congestion, allergies, or structural conditions like a deviated septum, the body shifts toward mouth breathing. Mouth breathing significantly increases the likelihood of drooling because it requires the mouth to remain open for airflow. This dual pathway of air and saliva reduces the effectiveness of natural swallowing reflexes during sleep.
In some cases, drooling may be indirectly associated with sleep disorders such as obstructive sleep apnea. Sleep apnea is characterized by repeated interruptions in breathing during sleep, often caused by partial airway collapse. Individuals with this condition may exhibit mouth breathing, snoring, and fragmented sleep. While drooling alone is not diagnostic of sleep apnea, its presence alongside other symptoms can sometimes indicate disrupted airway function that may require medical evaluation.
Gastroesophageal reflux disease can also influence nighttime saliva behavior. When stomach acid flows back into the esophagus, the body may respond by increasing saliva production as a protective mechanism to neutralize acidity. This increase in saliva can contribute to drooling, particularly when combined with relaxed swallowing during sleep.
From a neurological perspective, drooling reflects the broader reduction in voluntary control that occurs during sleep. The brain is not “off” during sleep; instead, it shifts into specialized modes of activity. Deep sleep supports physical restoration, tissue repair, and immune function, while REM sleep is heavily involved in memory consolidation and emotional regulation. In both states, the balance between control and relaxation shifts, allowing involuntary processes like saliva flow to become more visible.
Hydration status and general physiology can also influence drooling. Saliva production is affected by fluid balance in the body, and individuals with higher hydration levels may naturally produce more saliva. Certain foods, particularly those that are acidic or spicy, can stimulate salivary glands even hours after consumption. Medications that affect the nervous system or alter glandular activity may also increase or decrease saliva production, indirectly influencing drooling frequency.
Age is another important factor. In infants and young children, drooling is extremely common due to the ongoing development of neuromuscular coordination. Babies are still learning to coordinate swallowing, breathing, and tongue movement, and teething further increases saliva production. In adults, persistent or sudden changes in drooling patterns may be more noticeable because they deviate from established baseline behavior.
Dental structure and jaw alignment also contribute to how effectively the mouth remains closed during sleep. Misalignment of teeth, improper bite positioning, or temporomandibular joint issues can make it more difficult for the lips to seal completely. Even slight anatomical differences in jaw shape or tongue posture can influence whether saliva remains contained or escapes during sleep.
Despite its physiological basis, drooling often carries unnecessary social stigma. Many people associate it with loss of control or poor sleep hygiene, but in reality it frequently reflects the opposite: a state of deep relaxation where the body is fully disengaged from wakeful tension. In many cases, mild drooling can be interpreted as a sign that the nervous system has successfully transitioned into restorative sleep stages.
Sleep research increasingly supports the idea that small physical signals during sleep can provide meaningful insight into sleep quality. Technologies such as polysomnography and wearable sleep trackers measure brain waves, oxygen levels, muscle activity, and breathing patterns to better understand how different sleep stages affect bodily function. Within this framework, drooling is not a primary diagnostic marker, but it fits into a larger pattern of how muscle tone and airway control change overnight.
For individuals who find drooling bothersome, there are practical adjustments that can help reduce its occurrence. Changing sleep position, improving nasal airflow, addressing allergies, or using supportive pillows can all influence saliva flow during sleep. In some cases, improving overall sleep quality naturally reduces drooling by promoting more stable breathing patterns and better muscle coordination.
However, it is important to recognize that in most situations, drooling is completely harmless. It does not indicate neurological damage, disease, or dysfunction on its own. Only when accompanied by additional symptoms such as difficulty swallowing, chronic congestion, or severe sleep disruption does it warrant further medical attention.
Psychologically, understanding drooling from a scientific perspective can help reduce embarrassment. Many people are conditioned to view it as unpleasant simply because it is associated with loss of control. Yet sleep itself is a state defined by reduced conscious control. The body prioritizes repair, recovery, and maintenance over appearance or voluntary regulation. In that sense, drooling is simply a side effect of the body successfully entering a deeply restorative condition.
Ultimately, drooling during sleep is a small but revealing reminder of how complex and coordinated human physiology is even during rest. It reflects the interplay between brain activity, muscle relaxation, breathing patterns, and anatomical structure. Far from being a flaw, it is part of a broader system that allows the body to recover each night.
When viewed through this lens, drooling is not something to be ashamed of or ignored. It is a subtle indicator that the body is doing exactly what it is designed to do: enter a state of deep rest, reduce conscious control, and allow essential biological processes to take place uninterrupted.